Posted by: University Eye Specialists in Eye Health

Basic Monofocal Intraocular Lens (IOL) Implants
Basic monofocal intraocular lenses have a single focus and are generally offered in more than 50 different powers, from multiple manufacturers, which can be selected to focus your eye for either near, far, or in between, based on the precise dimensions and curvature of your eye. However, they only have a small focal range and cannot correct for astigmatism. They are a good choice for individuals who do not have much astigmatism and do not mind wearing glasses for near vision, or for those who are comfortable with wearing glasses to correct their astigmatism for both distance and near vision. They are the most common type of IOL used in cataract surgery and they are covered by your medical insurance, since an intraocular lens implant is necessary to focus light onto the retina for you to see with any clarity after cataract surgery.
Advanced Technology IOLs
- Toric
- Enhanced Monofocal/Toric
- Multifocal
- Extended Depth of Focus
- Light Adjustable Lens
What are Toric Monofocal Intraocular Lens (IOL) Implants?
Toric lens implants are one of the most popular technologies for cataract patients with astigmatism who do not want to always wear glasses. They are designed to improve how well you see without glasses at a distance, as compared to if you had a standard lens implant.
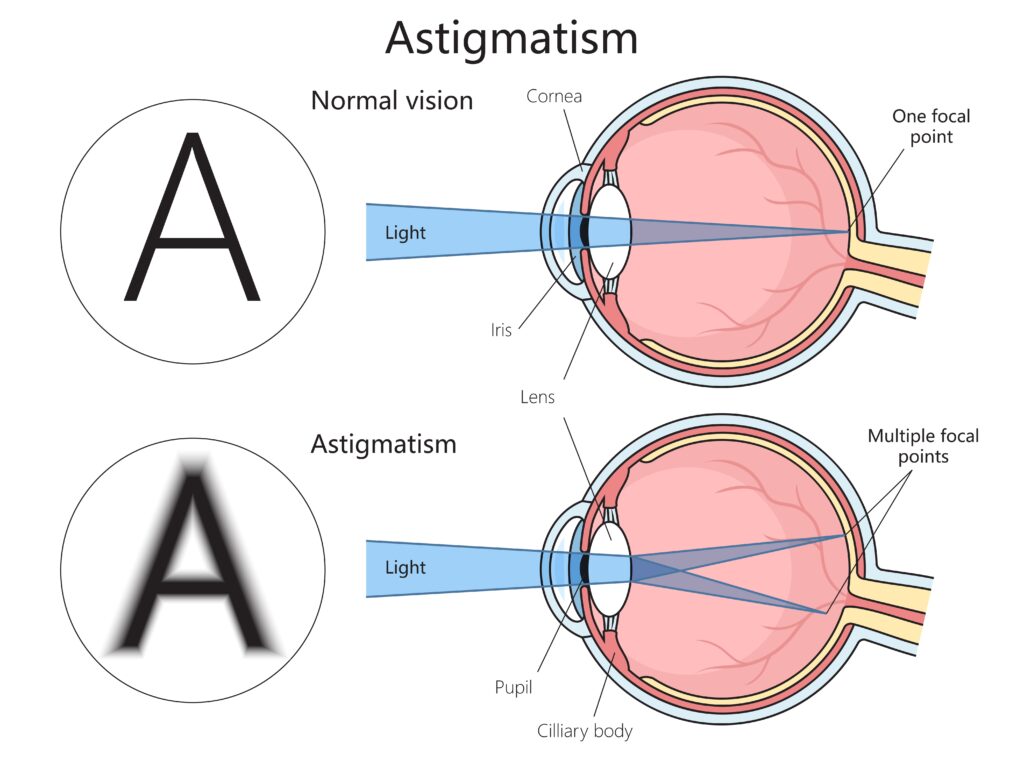
What Is Astigmatism?
Like nearsightedness or farsightedness, astigmatism describes a common type of natural blur that occurs to differing degrees in healthy eyes that can be corrected by wearing glasses. It results from an inherited, imperfect optical shape of the cornea, the clear front tissue of the eye. The perfect shape of your cornea would be if it were symmetric and perfectly curved in all directions, but humans generally have some asymmetry to their corneas. However, if this asymmetry is significant then it will cause the general shape to be more oblong (like the back of a teaspoon) instead of spherical, leading to defocus of light rays and blurrier vision compared to patients with smaller amounts astigmatism. Thus, the more astigmatism one has, the blurrier the vision is without glasses, and there is no advantage to astigmatism because it adds blur at every distance of focus. Corrective glasses or contacts can compensate for this corneal shape and optically correct the blur to properly focus an eye with astigmatism.
However, astigmatism can be reduced or nearly eliminated at the same time as cataract surgery using a toric IOL. By mapping your corneal shape with diagnostic technologies such as corneal topography and corneal tomography, we can calculate the amount of residual corneal astigmatism correction that your eye should require after surgery and incorporate the data into selecting the best lens for you prior cataract surgery. Toric lenses are only available in designated powers and therefore may not correct all the astigmatism, especially if it is severe. For lower amounts of astigmatism, where toric lenses are not available, corrective corneal microincisions, called LRIs, can be used to reduce your need for astigmatism correction after surgery. It is also important to understand that one’s current astigmatism is a product of both the cornea and the cataract, and therefore may change significantly once the cataract is removed, thus requiring correction of the remaining astigmatism with glasses or a toric IOL, even if perhaps this was not necessary before.
Glasses can be used to correct any small amount of astigmatism that remains after cataract surgery, if needed. In addition, toric lenses are now available in 3 different types of IOLs: Monofocal, Enhanced Monofocal, and Extended Range/Multifocal versions which increase the range of focus. However, there are no lenses available that will give you an adjustable focus with dedicated light energy at any distance, like that of a young person. Yet, despite the limits of technology, toric lens implants allow many patients to see better without the need to wear eyeglasses for correcting their astigmatism at all distances, and any eyeglasses worn will not need to be as strong as a result. For example, over the-counter reading glasses or non-prescription sunglasses should work much better if your astigmatism is minimized with a toric lens. Although it can increase slowly in some eyes with age, astigmatism will not go away on its own, and therefore the benefits of a toric lens implants should be lifelong.
Will I Still Need Glasses with A Toric Lens Implant?
The monofocal toric lens implant does NOT allow you to both read and see far away without glasses. It may not necessarily correct 100% of your astigmatism either. However, compared to a basic lens implant that does not correct astigmatism, the toric lens implant should improve how well you see without glasses, and any eyeglasses that you do require should be less strong, less expensive, and likely more comfortable to wear.
Much like contact lenses or glasses, every intraocular lens implant model (both standard, toric, multifocal, and light adjustable) is manufactured in different strengths of dioptric power. Generally, these are offered in more than 50 different base “powers” by each manufacturer for each of their different models. However, even with this large number of intraocular lenses, they still account for less than half the number of potential glasses lens combinations available, and as a result, limit how exacting the focal target selection can be with every lens, except the Light Adjustable Lens. This is why many surgeons will refer to the selecting of an intraocular lens as an art and a science.
As you might expect, precise preoperative measurements are very important in selecting the appropriate intraocular lens implant power for your eye and the target focus. In order to prescribe the correct spectacles or contact lens power, a trial and-error approach, whereby you get to preview various lens powers in front of your eye is performed. This is why you are asked, “Which is better, one or two?” during an eye exam, as you are incrementally selecting which of the two lens powers that you see best with to arrive at a final “best” lens focus. However, because intraocular lens implants are inserted inside the eye at the time of surgery, once your anatomical lens (cataract) has been removed, it is impossible for you to preview or “try out” different powers during the surgery. Likewise, it cannot simply be switched to a different lens implant power later, as one could with glasses or contact lenses.
Fortunately, the appropriate power of the lens implant can be closely estimated using mathematical formulas and calculations based on the preoperative measurements of your eye. Although these measurements are very accurate, there are individual variables that prevent this process from being 100% perfect. One important variable is the precise final positioning of the intraocular lens implant inside the lens capsule once healing is complete. The entire process is accurate enough that most patients will see quite well without glasses in the distance (assuming this was the target). Frequently, the target is not “absolutely perfect,” and you might choose to wear thin glasses with a mild prescription for those times when a sharper focus is required. Recently, the option of using LAL technology (see LAL section) is available and will allow some patients to fine tune or adjust their lens’s focus after surgery.
What are different Lifestyle Lenses?
Intraocular lenses have traditionally been either monofocal or multifocal, with toric correction additionally available for either. However, more recent advancements in lens technology have brought the release of “Enhanced Monofocal” lenses such as the TECNIS Eyhance™ and RayOne EMV to the monofocal category. Previously, monofocal intraocular lenses only corrected vision to help patients with cataracts see things at a single distance and thus did not improve the intermediate vision that is required for many important daily tasks. These so-called “Lifestyle Lenses” are the newest generation IOLs and are designed to extend the depth of field to provide enhanced intermediate vision, but with only minimal effects on distance vision. These lenses enable most patients to perform certain activities requiring intermediate vision with greater ease, and to engage in activities of interest, including favorite hobbies such as cooking or reading a mobile device.
Can the Eyhance™ and EMV IOLs Correct My Astigmatism?
The TECNIS Eyhance™ lens is available in a toric and non-toric IOL model for correcting astigmatism when necessary, and the Rayner RayOne EMV is currently only available as a non-toric IOL (the toric model is expected soon). Lower amounts of astigmatism can be combined with a micro-CRI, for astigmatism control at the time of surgery, using the non-toric models for enhanced intermediate vision as well.
Will Insurance Cover the Cost Of An Advanced Technology Lens?
Unfortunately, Medicare and most other insurances will only pay for cataract surgery with a standard monofocal lens. Thus, there is an additional cost for any of the Advanced Technology IOLs, but the potential to reduce dependence on prescription glasses can be of significant benefit for some. If you are interested in any of the Advanced Technology IOLs, such as a Toric, Multi Focal, Light Adjustable, or enhanced monofocal lens like the TECNIS Eyhance™ or RayOne EMV, please let your surgeon know. Your insurance will pay for the surgical fee, the outpatient facility fee, and the anesthesia fee, but you will need to pay out-of-pocket for the Advanced Technology Lens, if selected.
How Is Vivity® Different from Multifocal (Bifocal or Trifocal) Intraocular Lenses?
Alcon Vivity® uses a new, non-diffractive technology called X-Wave™. This is Alcon’s proprietary, non-diffractive wavefront technology which creates a “continuous extended range of vision for distance and intermediate tasks with functional near vision.” Other diffractive multifocal lenses split the wavefront into multiple separate focal zones using concentric rings on the surface of the IOL. The Vivity IOL can be chosen in “natural” coloration to filter blue light rays, if selected. Patients with other multifocal lenses may complain about visual disturbances such as halos and glare, which are a function of the common multifocal “concentric ring” architecture. Some patients will opt for monofocal lenses simply because they have a much lower rate of these visual side effects postoperatively. However, patients with Vivity intraocular lenses reported lower visual disturbances when compared to traditional multifocal IOLs, with incidences closer to those seen with monofocal lenses. This is a distinct advantage for patients wanting to be able to drive at night while also increasing their functional near ability without corrective glasses. As with multifocal IOLs, some patients will not be good candidates for these lenses due to corneal aberrations or preexisting ocular conditions.

Will I Still Need Reading Glasses After Getting Vivity Lenses?
Reading glasses may still be necessary for fine print or prolonged reading. Most patients achieve excellent visual acuity, meaning their vision is sharper for distance and intermediate vision in both bright and dim lighting, although reading in dim lighting can still be challenging because of pupil size. Many patients with Vivity lenses are able to check a message on their smartphone or read a label at the store without glasses, but may need their glasses to do fine, detailed work.
Can Vivity® Be Used If I Have Astigmatism or Other Eye Conditions?
The Vivity lens is available in a toric IOL model so that regular astigmatism can be corrected at the time of cataract surgery. Multifocal lenses do not work well unless the patient has eyes that are in excellent shape. This means that they have no issues like dry eye syndrome, corneal scars or significant corneal or macular irregularity. So far, ophthalmologists are reporting that they have used Vivity with success in patients with glaucoma, as well as patients with some macular disorders. Your ophthalmologist can evaluate whether you are a good candidate for a Vivity® IOL.
How Are Trifocal IOLs Different from Other Multifocal IOLs?
The Alcon PanOptix® lens was the first trifocal lens to be released in 2019 and uses an optical technology ENLIGHTEN® to optimize intermediate vision without compromising near and distance vision, to give three distinct areas of extended range of vision with reduced glasses dependence. The Johnson & Johnson Odyssey lens builds upon the Echelette trifocal design, using their OptiBlue® platform to filter violet light, soften echelette transitions to reduce the halo effect caused by multifocal technology and correct chromatic aberration for better contrast3,4. The PanOptix® is available in both non-toric and toric option for astigmatism correction, while the Odyssey, released in early 2024, does not have a toric yet released. Given that there are three distinct areas in focus, these lenses allow for a greater range of glasses independence than previous multifocal IOLs, although more time for neuroadaptation may be required. Also similar to other multifocals, bilateral use when a short period of time is recommended to allow for full functionality. The concentric ring design does have a higher incidence of glare and halos than basic monofocal IOLs, and thus may not be a good choice for those who often drive at night. Properly selected PanOptix® and Odyssey IOL patients can, for instance, read menus (near vision), work at their computer (intermediate vision), or play golf (far vision) with relative ease. As with other multifocal IOLs, some patients will not be good candidates for these lenses due to corneal aberrations or preexisting ocular conditions.
What are Light Adjustable Lens (LAL)™?
The RxSight Light Adjustable Lens™ is the first and only intraocular lens that can be adjusted for fine tuning of the patient’s preferred primary focus after implantation. Using a special macromere matrix within the lens material designed by a Nobel Prize-winning scientist, RxSight has developed the first intraocular lens (IOL) that allows you and your physician to optimize your vision following cataract surgery. Despite numerous advances in modern cataract surgery technologies, only 6 out of 10 cataract patients achieve their targeted vision, and an even smaller percentage achieve excellent vision at all distances. ¹ This is because it is very difficult to predict how your eye will heal before your cataract surgery. With the Light Adjustable Lens, you can now customize your vision after your cataract surgery. You will have the unique ability to adjust and preview your vision to assure it meets your personal preferences and lifestyle requirements. This optimization is done after lens implantation through a series of light treatment procedures in the office that take only a few minutes each. The Light Adjustable Lens delivers superior visual outcomes that nonadjustable IOLs cannot match.² In a study of 600 subjects, those who received the Light Adjustable Lens followed by adjustments were twice as likely to achieve 20/20 distance vision at 6 months without glasses as those who received a standard monofocal IOL.
How Does the Light Adjustable Lens Work?
The Light Adjustable Lens is made of a special photosensitive material that changes the shape and power of your implanted lens in response to ultraviolet (UV) light in a precise configurable pattern. Light treatments are painless and are delivered with the Light Delivery Device (LDD) machine in the office over a few minutes.

The Light Adjustable Lens is the only adjustable intraocular lens (IOL) available that allows optimization of your vision after lens implantation and healing. If you and your doctor select the Light Adjustable Lens, the first step is to have your cataract safely removed and the adjustable IOL implanted. The cataract removal and IOL implantation procedure is the same as if you selected a non-adjustable IOL.
What is unique about the Light Adjustable Lens is that once your eye has healed, you return to your eye doctor to have your vision tested. During this visit you will be able to preview and compare possible vision outcomes based on your unique preferences and lifestyle requirements before selecting a prescription for your adjustable lens. The doctor will then apply a proprietary light treatment that precisely reshapes your implanted lens based on the visual correction that is needed to target your custom prescription. You’re allowed to “test drive” the vision for several days prior to returning for further light treatment or locking in of your vision once your elected target is achieved. You may need 3 to 5 total light treatments, per eye, to reach your vision goals.
Is The RxSight Light Adjustable Lens™ Right for Me?
The U.S. Food and Drug Administration has approved the Light Adjustable Lens and Light Delivery Device for patients with preexisting astigmatism of at least 0.50 diopters or more who are undergoing cataract surgery. Other IOLs may be available for the treatment of your cataracts and your doctor will help you determine which lens is right for you and if a LAL may be a good choice for your best visual outcome.
What To Expect Following Your Cataract Surgery with A Light Adjustable Lens™?
After your Light Adjustable Lens™ has been implanted in your eye, it is adjusted to deliver the customized vision you desire. This means that there are 2 major differences following your surgery as compared to a non-adjustable intraocular lens (IOL):
- Required wear of ultraviolet (UV) protective glasses at all times.
- Completion of light treatments after 3-4 weeks from surgery with around 3-5 in-office treatment sessions per eye.
Why Do I Need to Wear Protective Glasses?


Exposure to indoor and outdoor sources of UV light can cause uncontrolled changes to the Light Adjustable Lens. To prevent this, you will be provided with UV protective glasses to wear immediately following surgery during waking hours (from the time of lens implantation until after the last light treatment is completed).
Your protective glasses may be removed when sleeping and may be temporarily removed when showering, washing your face, or applying eye drops as long as you are not exposed to direct sunlight. Twenty-four hours after your final light treatment, no further changes can be made to the implanted Light Adjustable Lens, and you can remove the UV protective glasses and enjoy your custom vision!
How Are the Light Treatments Performed?
To receive the light treatment, you will be placed in front of the Light Delivery Device (LDD). The LDD non-invasively delivers UV light to your Light Adjustable Lens to adjust your vision to the desired target. The system gives the flexibility to make adjustments and refinements to meet your specific criteria. Following the light treatment, you will be rechecked in approximately 3-7 days to assess your vision.
Between 3 and 5 total light treatments per eye, each lasting approximately 90 seconds and separated by approximately 3-7 days, is required. The total number of light treatments is based on the achievement of the desired target focus that you and your doctor selected. When you are able to experience the results of your adjustments, you will better understand the value of adjusting and customizing your vision after your surgery. Once you have achieved your optimal vision, the lens power is permanently locked in with a final light treatment to prevent any further changes.
LIGHT TREATMENT SCHEDULE
- Initial Light Treatment: Approximately 3-4 weeks after surgery.
- Secondary Light Treatment: Approximately 3-7 days after initial light treatment.
- Additional Light Treatments (as required): Approximately 3-7 days after each prior light treatment.
- Market Scope 2020 IOL Market Report: A Global Analysis for 2019 to 2025.
- US Food and Drug Administration. Summary of Safety and Effectiveness (SSED) of Light Adjustable Lens and Light Delivery Device System. 3. ARVO 2020_Effect of Blocking Violet Light in Extended Depth of Focus IOL:SC2019CT4056.
- Effects of blocking violet light in EDOF IOLs. JNJ ARVO Abstract May 2020/Optical and Visual performance violet blocking IOL:SC2019CT4025.